Polymyalgia rheumatica (PMR) is an inflammatory disease characterized by severe aching of the shoulders, hips, and neck with associated morning stiffness which presents in older adults. The classic symptoms include:
- Pain and tenderness in the shoulders, hips, and neck
- Morning stiffness
- Fever, malaise, and generalized weakness
In the past, PMR was believed to be a type of rheumatoid arthritis in the aging population, however, the two conditions are different. Unlike RA, PMR does not cause permanent joint damage and does not typically affect the hands, wrists, knees, or feet.
See Is My Joint Pain Caused by Rheumatoid Arthritis (RA) or Another Autoimmune Disorder?
Who Gets Polymyalgia Rheumatica?
Polymyalgia rheumatica is the most common inflammatory disease affecting the age group above 50 years. The risk of PMR rises with age, and the average age at diagnosis is about 75 years. 1 Mackie SL. Polymyalgia rheumatica: pathogenesis and management. Clinical Medicine [serial online]. August 2013;13(4):398-400. Women are approximately 2 to 3 times as likely to be affected as men. 2 Michet Clement J, Matteson Eric L. Polymyalgia rheumatica BMJ 2008; 336 :765
In This Article:
How Does Polymyalgia Rheumatica Cause Joint Pain?
Diagnostic imaging such as ultrasonography, magnetic resonance imaging (MRI), and positron emission tomography (PET) scans present a detailed picture of what goes on in the anatomy of the affected joints during the development of PMR. Imaging shows inflammation of synovial membrane tissue that is commonly found in bursae, joints, and tendons. This inflammation causes pain.
The main types of inflammation associated with PMR include:
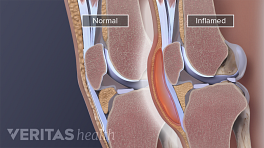
- Bursitis. PMR often causes bursitis in the shoulder, hip, and neck joints. Bursitis is the inflammation of a bursa. A normal bursa is a tiny fluid-filled sac that functions to reduce friction and ensure smooth movement between the bone and the surrounding tissues, such as muscles, ligaments, tendons, and other soft tissues adjacent to the bone. Normally, the bursa is lined by a synovial membrane and contains small amounts of fluid. In bursitis, the membrane of the sac is inflamed, and there is fluid buildup inside the sac, causing pain.
- Synovitis. The shoulder and hip joints may be affected by a condition called synovitis. A normal synovial joint is surrounded by a synovial membrane. During synovitis, this membrane gets inflamed, and synovial fluid collects inside the membrane. The inflammation and swelling cause pain during joint movement.
- Tenosynovitis. Tendon sheaths are the outer covering of tendons, and are also made of synovial membrane tissue, which are prone to inflammation in PMR. This inflammation of the synovial membrane of tendon sheaths is called tenosynovitis.
The exact cause of inflammation of the synovial membrane tissue in PMR is not known. Research suggests that genetics, environmental factors, and infectious agents play a role in the development of joint inflammation in PMR.
Long-Term Outlook for People with PMR
Polymyalgia rheumatica can be a self-limiting condition, which means it is not permanent and can resolve itself over a period of time. 3 Kyle V, Hazelman BL. Editorial: Stopping steroids in polymyalgia rheumatica and giant cell arteritis. BMJ 1990;300:344–5. As cited in - Charlton R. Polymyalgia rheumatica and its links with giant cell arteritis. Clin Med 2008;8:498–501. However, the symptoms of PMR can be quite severe and require treatment. PMR is usually treated for about 2 years, though studies have shown it can last up to 7 years. 3 Kyle V, Hazelman BL. Editorial: Stopping steroids in polymyalgia rheumatica and giant cell arteritis. BMJ 1990;300:344–5. As cited in - Charlton R. Polymyalgia rheumatica and its links with giant cell arteritis. Clin Med 2008;8:498–501. , 4 Behn AR, Perera T, Myles AB. Polymyalgia rheumatica and corticosteroids: how much for how long?Ann Rheum Dis 1983;42:374–8. , 5 Dasgupta B., Borg FA., Hassan N. et al. on behalf of the BSR and BHPR Standards, Guidelines and Audit Working Group; BSR and BHPR guidelines for the management of polymyalgia rheumatica, Rheumatology, Volume 49, Issue 1, 1 January 2010, Pages 186–190. , 6 Kyle V, Hazleman BL. Treatment of polymyalgia rheumatica and giant cell arteritis. II. Relation between steroid dose and steroid associated side effects. Annals of the Rheumatic Diseases. 1989;48(8):662-666. Unlike other forms of joint inflammatory conditions, PMR does not cause progressive or permanent damage or disability to the muscles and joints.
Relationship of PMR with Giant Cell Arteritis
PMR is frequently associated with giant cell arteritis, also known as temporal arteritis. Giant cell arteritis is a serious condition and can cause complications such as permanent blindness. This condition causes an inflammation of blood vessels supplying the scalp, eyes, and other larger blood vessels supplying other parts of the body. Expert analysis indicates approximately 9% to 20% PMR cases eventually develop giant cell arteritis. 7 Gonzalez-Gay MA. Giant cell arteritis and polymyalgia rheumatica: two different but often overlapping conditions. Semin Arthritis Rheum 2004 Apr; 33 (5): 289-93 As cited in - Schmidt J, Warrington K. Polymyalgia Rheumatica and Giant Cell Arteritis in Older Patients. Drugs & Aging [serial online]. August 2011;28(8):651-666.
- 1 Mackie SL. Polymyalgia rheumatica: pathogenesis and management. Clinical Medicine [serial online]. August 2013;13(4):398-400.
- 2 Michet Clement J, Matteson Eric L. Polymyalgia rheumatica BMJ 2008; 336 :765
- 3 Kyle V, Hazelman BL. Editorial: Stopping steroids in polymyalgia rheumatica and giant cell arteritis. BMJ 1990;300:344–5. As cited in - Charlton R. Polymyalgia rheumatica and its links with giant cell arteritis. Clin Med 2008;8:498–501.
- 4 Behn AR, Perera T, Myles AB. Polymyalgia rheumatica and corticosteroids: how much for how long?Ann Rheum Dis 1983;42:374–8.
- 5 Dasgupta B., Borg FA., Hassan N. et al. on behalf of the BSR and BHPR Standards, Guidelines and Audit Working Group; BSR and BHPR guidelines for the management of polymyalgia rheumatica, Rheumatology, Volume 49, Issue 1, 1 January 2010, Pages 186–190.
- 6 Kyle V, Hazleman BL. Treatment of polymyalgia rheumatica and giant cell arteritis. II. Relation between steroid dose and steroid associated side effects. Annals of the Rheumatic Diseases. 1989;48(8):662-666.
- 7 Gonzalez-Gay MA. Giant cell arteritis and polymyalgia rheumatica: two different but often overlapping conditions. Semin Arthritis Rheum 2004 Apr; 33 (5): 289-93 As cited in - Schmidt J, Warrington K. Polymyalgia Rheumatica and Giant Cell Arteritis in Older Patients. Drugs & Aging [serial online]. August 2011;28(8):651-666.